
Abstract
This de-identified case study examines psychological, neurocognitive, and neurophysiological recovery in a 72-year-old Hispanic male Vietnam combat veteran, firefighter-EMT, and coroner following three sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR). The participant presented with severe posttraumatic stress symptoms (PCL-5 = 60), severe depressive symptoms (PHQ-9 = 21), and severe anxiety (GAD-7 = 18), along with decades of cumulative trauma exposure from combat, emergency response, death investigation, and the traumatic loss of his daughter in a motor vehicle fatality while simultaneously attempting life-saving measures on his granddaughter.
Baseline assessment using the Evoke Neuroscience platform revealed impaired global neurocognitive performance (53%), executive dysfunction, affect dysregulation, severe autonomic suppression, and cortical hyperactivation consistent with chronic trauma burden. Following three TRP-PR sessions, post-treatment symptom scores decreased to zero across all measures. Neurocognitive global performance improved to 88%, autonomic function improved substantially, and quantitative electroencephalography (quantitative EEG (qEEG)) findings demonstrated reduced cortical hyperactivation and improved network efficiency.
This case suggests that TRP-PR may facilitate rapid and meaningful recovery in individuals with layered, lifelong trauma exposure, even in older adulthood.
Keywords: combat trauma, moral injury, cumulative trauma, Vietnam veteran, first responder, TRP-PR, quantitative EEG (qEEG), heart rate variability (HRV) https://healingthehero.org/research/
Table of Contents

1. Introduction and Literature Review
Note: This manuscript is a de-identified clinical case study intended to describe observed pre/post changes in a single participant, one of 30 Firefighters and 45 Veterans in the ASU study. Findings should be interpreted a descriptive and hypothesis-generating rather than definitive evidence of efficacy until the study is concluded.
Trauma exposure among combat veterans and first responders is both frequent and cumulative, often resulting in long-term psychological, neurobiological, and functional consequences. These populations routinely face life-threatening events, moral injury, repeated exposure to death, and chronic occupational stress. The interaction between these exposures and the brain’s stress-response systems can produce enduring changes in emotional regulation, autonomic nervous system function, cognitive processing, and overall quality of life.
Combat Veterans: Chronic Effects of War-Related Trauma
Combat veterans represent one of the most extensively studied populations in trauma research. The U.S. Department of Veterans Affairs (VA) estimates that PTSD affects a substantial proportion of veterans, with prevalence rates varying by era of service, combat intensity, and cumulative exposure. Among Vietnam veterans, lifetime PTSD prevalence has been reported to range from approximately 11% to 30%, with many individuals continuing to experience symptoms decades after combat exposure (VA, 2019).
Vietnam veterans are uniquely affected because many experienced prolonged exposure to ambushes, death, severe injury, survivor guilt, and difficult reintegration. Chronic combat trauma can alter limbic activation, prefrontal regulation, hippocampal memory processing, and autonomic flexibility.
Moral Injury and Combat Trauma
Beyond fear-based trauma, many veterans carry moral injury—psychological distress stemming from actions, inactions, or witnessed events that violate deeply held moral beliefs. Moral injury may manifest as shame, guilt, grief, existential distress, and self-condemnation (Litz et al., 2009).
Firefighters, EMTs, and Coroners: Cumulative Occupational Trauma
Firefighters, paramedics, and coroners face repeated exposure to severe bodily injury, traumatic deaths, pediatric fatalities, rescue failures, and mass casualty incidents. The CDC and NIOSH recognize first responders as high-risk populations for PTSD, depression, sleep disorders, substance misuse, and suicide.
Repeated exposure to death can profoundly affect emotional processing, worldview, family functioning, and physiological stress regulation. Coroners and death investigators are particularly vulnerable due to chronic exposure to violent death scenes and cumulative grief load.
Relevance to the Present Case
The present case is clinically significant because it reflects unresolved combat trauma from Vietnam, decades of trauma exposure as a firefighter-EMT and coroner, and the traumatic death of a daughter in a traffic fatality while the participant simultaneously attempted life-saving measures on his granddaughter.
This layered trauma history likely contributed to chronic hyperarousal, emotional burden, altered threat processing, and impaired autonomic flexibility.
2. Case Presentation
Participant
The participant was a 72-year-old Hispanic male with a history of:
- combat service as an infantryman in Vietnam,
- service as a firefighter-EMT,
- service as a coroner / death investigator.
Trauma History
The participant carried cumulative trauma across multiple decades and roles:
- combat-related threat, loss, and repeated life-or-death stress in Vietnam,
- repeated occupational exposure to severe injuries, fatalities, and human suffering,
- the traumatic loss of his daughter in a motor vehicle crash,
- simultaneous life-saving efforts for his granddaughter at the scene.
This trauma burden was consistent with chronic unresolved grief, cumulative occupational trauma, and long-term autonomic dysregulation.
Pre-Treatment Psychometric Symptoms
- PCL-5: 60
- PHQ-9: 21
- GAD-7: 18
Post-Treatment Psychometric Symptoms
- PCL-5: 0
- PHQ-9: 0
- GAD-7: 0
The participant completed three sessions of TRP-PR between baseline and follow-up assessment.
3. Method
Measures
Psychometric:
- Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5)
- Patient Health Questionnaire-9 (PHQ-9)
- Generalized Anxiety Disorder-7 (GAD-7)
Neurophysiological:
- Evoke Neuroscience quantitative EEG (qEEG)
- Event-Related Potentials (ERP)
- ECG-derived Heart Rate Variability (heart rate variability (HRV))
- Neurocognitive screener
Procedure
The participant completed baseline psychometric and Evoke Neuroscience assessments. He then completed three sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR), a structured intervention designed to reduce the emotional intensity associated with unresolved traumatic experiences without requiring prolonged narrative exposure. Follow-up psychometric and neurophysiological assessments were completed post-intervention.
4. Results: Neurocognitive Recovery
Global Neurocognitive Performance
- Pre-treatment global score: 53%
- Post-treatment global score: 88%
Domain-Level Changes
| Domain | Pre | Post | Change |
| Memory | 65% | 95% | +30 |
| Executive / Attention | 46% | 83% | +37 |
| Word Fluency | 50% | 88% | +38 |
| Affect | 42% | 83% | +41 |
| Sensory | 38% | 71% | +33 |
| Motor | 46% | 88% | +42 |
These findings indicate broad recovery in emotional regulation, executive function, language output, and sensorimotor integration.
5. Results: Response Metrics and ERP Findings
Response Metrics
Pre-treatment:
- Reaction time: 474ms
- Variability: 12ms
- Omission errors: 0%
- Commission errors: 6.12%
Post-treatment:
- Reaction time: 547ms
- Variability: 5ms
- Omission errors: 0%
- Commission errors: 2.45%
Interpretation: Post-treatment performance was more accurate and consistent, suggesting improved inhibitory control and attentional stability despite slightly slower response speed.
ERP Findings
P300a ERP (Attention)
- Pre: 312ms / 4.9 microvolts
- Post: 640ms / 14.3 microvolts
P300b ERP (Working Memory Updating)
- Pre: indiscernible
- Post: indiscernible
N100 ERP (Sensory Processing)
- Pre: 292ms / -27.9 microvolts
- Post: 276ms / -17.2 microvolts
Interpretation: Post-treatment findings suggest stronger attentional engagement and improved sensory gating, with persistent deeper working memory inefficiencies likely reflecting age and cumulative trauma burden.
6. Results: heart rate variability (HRV) and Autonomic Recovery
Heart Rate Variability (HRV) Changes
| Metric | Pre | Post |
| Heart Rate | 88 bpm | 70 bpm |
| SDNN | 17ms | 60ms |
| Total Power | 129 ms^2 | 621 ms^2 |
| QRS | 0.155 sec | 0.125 sec |
Interpretation
The participant demonstrated marked improvement in autonomic regulation, including:
- lower resting physiological arousal,
- improved vagal tone,
- increased autonomic flexibility,
- improved cardiovascular recovery capacity.
These changes strongly support meaningful physiological recovery rather than subjective symptom change alone.
7. Results: quantitative EEG (qEEG) Brain Map Findings
Pre-Treatment quantitative EEG (qEEG)
Findings included:
- theta-to-beta ratio: 2.110
- posterior excess activity,
- precuneus hyperactivation,
- middle / superior temporal excess,
- medial frontal hyperactivation,
- cuneus excess.
Interpretation: This pattern was consistent with chronic trauma-linked hypervigilance, internal threat monitoring, emotional overcoupling, and persistent memory-related cortical burden.
Post-Treatment quantitative EEG (qEEG)
Findings included:
- theta-to-beta ratio: 2.021 (normalized)
- improved cortical organization,
- reduced widespread excess activation,
- residual mild posterior / temporal elevations.
Interpretation: Post-treatment brain mapping suggests reduced cortical threat load and improved neural efficiency.
8. Discussion
This case demonstrates substantial multidomain recovery following three TRP-PR sessions in an older adult with severe cumulative trauma exposure.
Key findings included:
- complete remission of self-reported PTSD, depression, and anxiety symptoms,
- improved neurocognitive performance,
- better affect regulation,
- improved executive control,
- substantial autonomic recovery,
- reduced cortical hyperactivation.
The participant’s trauma burden was notable not only for its severity but also for its duration. He carried combat trauma from Vietnam, decades of occupational trauma, and profound personal grief. The degree of recovery observed suggests that targeted trauma processing may still produce meaningful neurophysiological change even after decades of unresolved burden.
This case is especially relevant to:
- aging combat veterans,
- retired first responders,
- individuals with layered cumulative trauma.
Limitations
This report is limited by its single-case design, the absence of a control condition, and the lack of long-term follow-up data within the present manuscript. Although the observed changes are substantial, conclusions should remain appropriately cautious. Additional research is needed to determine durability of outcomes, generalizability, and comparative effectiveness relative to other trauma interventions.
9. Conclusion
Conclusion
This de-identified case demonstrates that Trauma Resiliency Protocol–Peer Rescue (TRP-PR) may facilitate rapid and meaningful recovery in individuals with layered combat, occupational, and personal trauma.
After only three sessions, this participant showed:
- full symptom remission,
- improved cognitive functioning,
- improved autonomic regulation,
- reduced trauma-linked cortical burden.
These findings support continued structured investigation into TRP-PR as a rapid-response trauma intervention for veterans and first responders.
Appendix
Appendix A: Pre- and Post-Intervention Visual Data Summary
Figure A1. Pre-Intervention Evoke Neuroscience Brain Map
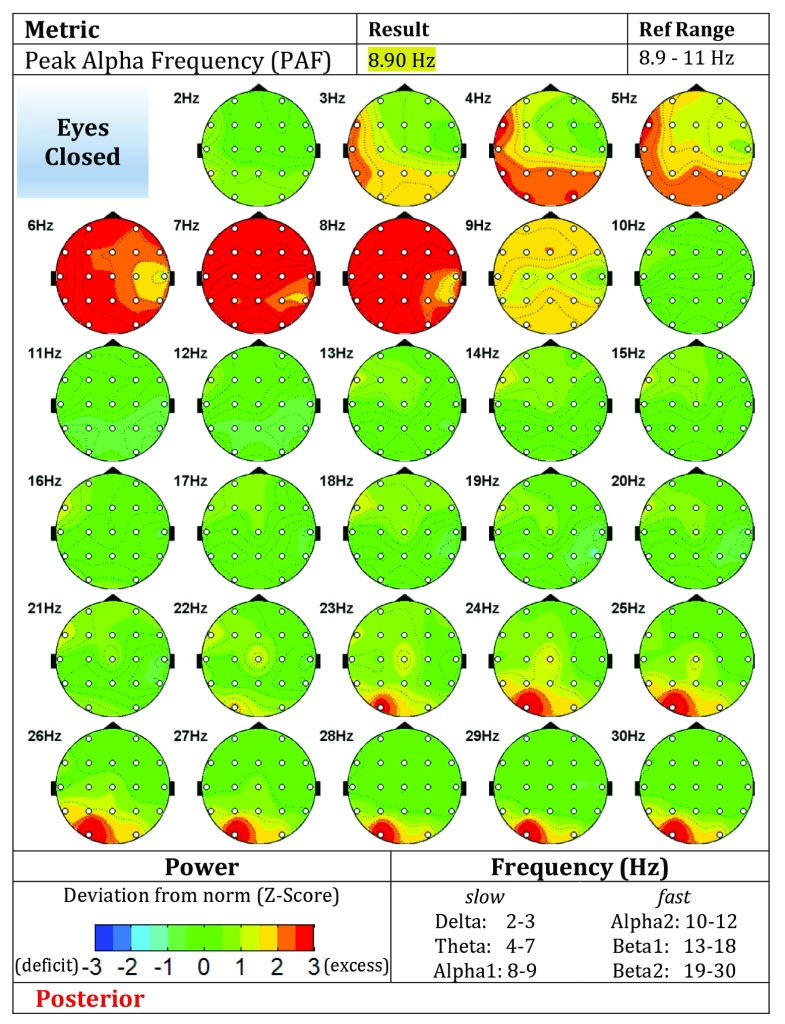
Caption: Baseline Evoke Neuroscience brain maps demonstrating posterior, temporal, and frontal excess activation patterns consistent with chronic trauma burden, hypervigilance, emotional overcoupling, and cumulative stress load.
Figure A2. Post-Intervention Evoke Neuroscience Brain Map
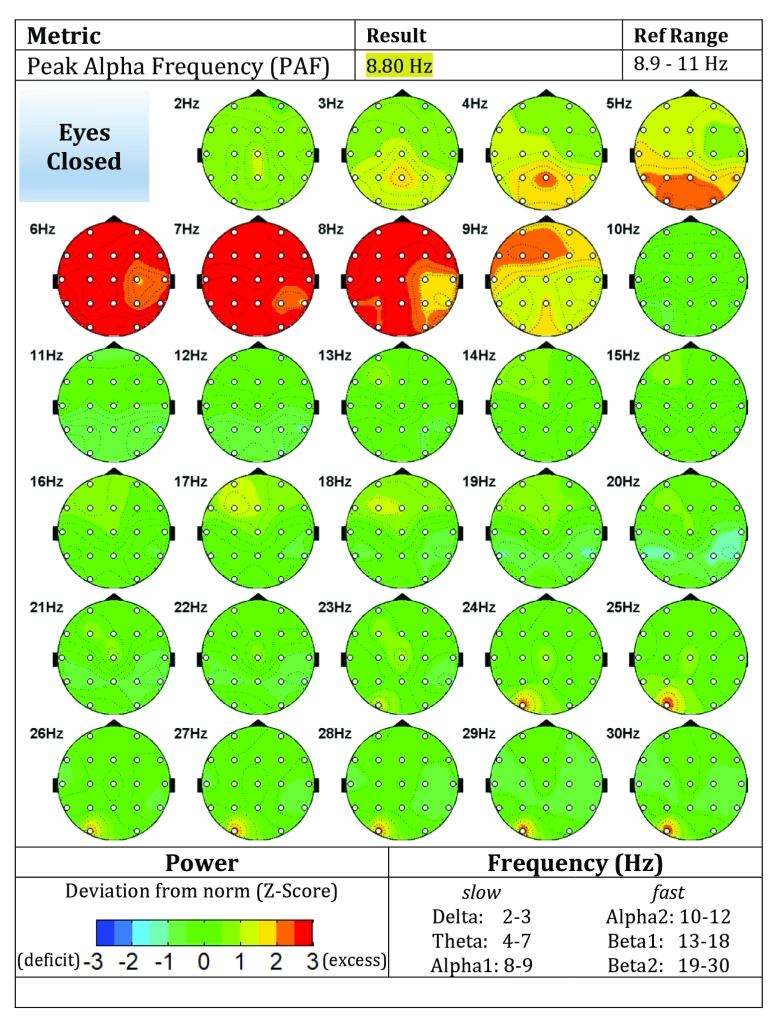
Caption: Post-treatment Evoke Neuroscience brain maps demonstrating improved cortical organization, reduced excess activation, and more efficient neural network regulation following three sessions of TRP-PR.
Table A1. Pre- and Post-Treatment Psychometric Outcomes
| Measure | Pre-Treatment | Post-Treatment | Clinical Change |
| PCL-5 | 60 | 0 | Full symptom remission |
| PHQ-9 | 21 | 0 | Full symptom remission |
| GAD-7 | 18 | 0 | Full symptom remission |
Table A2. Pre- and Post-Treatment Neurocognitive Outcomes
| Domain | Pre-Treatment | Post-Treatment | Change |
| Global Score | 53% | 88% | +35 |
| Memory | 65% | 95% | +30 |
| Executive / Attention | 46% | 83% | +37 |
| Word Fluency | 50% | 88% | +38 |
| Affect | 42% | 83% | +41 |
| Sensory | 38% | 71% | +33 |
| Motor | 46% | 88% | +42 |
Table A3. Pre- and Post-Treatment Autonomic Outcomes
| Metric | Pre-Treatment | Post-Treatment | Interpretation |
| Heart Rate | 88 bpm | 70 bpm | Improved resting arousal |
| SDNN | 17 ms | 60 ms | Improved autonomic flexibility |
| Total Power | 129 ms^2 | 621 ms^2 | Improved autonomic reserve |
| QRS Duration | 0.155 sec | 0.125 sec | Improved cardiac conduction |
Appendix Note
The appendix is intended to provide visual and quantitative support for the psychometric, neurocognitive, autonomic, and electrophysiological changes described in the main manuscript.
References
Beaton, R. D., & Corneil, W. (1999). Exposure to traumatic incidents and prevalence of posttraumatic stress symptomatology in urban firefighters in two countries. Prehospital and Disaster Medicine, 14(2), 102–108.
Brondolo, E., Clifton, C., Delahanty, D., Eftekharzadeh, P., & Schwartz, J. E. (2018). Work-related trauma, alienation, and posttraumatic and depressive symptoms in medical examiner employees. International Journal of Emergency Mental Health and Human Resilience, 20(6), 1–11.
Evoke Neuroscience. (n.d.). Evoke EEG system documentation.
Litz, B. T., Stein, N., Delaney, E., Lebowitz, L., Nash, W. P., Silva, C., & Maguen, S. (2009). Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clinical Psychology Review, 29(8), 695–706.
National Center for PTSD. (n.d.). What is PTSD? U.S. Department of Veterans Affairs. https://www.ptsd.va.gov/understand/what/index.asp
National Institute for Occupational Safety and Health. (2021). Suicides among first responders: A call to action. Centers for Disease Control and Prevention. https://www.cdc.gov/niosh/bulletin/2021/suicides-first-responders.html
U.S. Department of Veterans Affairs. (2019). How common is PTSD in veterans? https://www.ptsd.va.gov/understand/common/common_veterans.asp
Article by: Dan Jarvis | Founder of TRUSA, 22ZERO and Healing the Hero.
