Analysis of Neurofeedback for Healing: Traumatic Brain Injury
This provides an in-depth exploration of how Neurofeedback can be used to heal traumatic brain injury (TBI), drawing on extensive research and clinical insights to offer a detailed understanding for readers seeking a thorough analysis of Neurofeedback. The content expands on the overview, incorporating detailed findings, citations, and practical considerations, ensuring a comprehensive discussion.
Introduction
Traumatic brain injury (TBI) is a significant public health issue, affecting millions annually, with causes ranging from falls to motor vehicle accidents and sports injuries. The Centers for Disease Control and Prevention (CDC) reports that TBI contributes to a substantial number of emergency department visits, hospitalizations, and deaths, with long-term consequences including cognitive impairments, emotional disturbances, and physical disabilities (Traumatic Brain Injury & Concussion). Traditional treatments, such as pharmacological interventions and physical therapy, address symptoms but often fall short in restoring full brain function. Neurofeedback, a form of biofeedback utilizing electroencephalography (EEG) to provide real-time feedback on brainwave activity, has emerged as a potential complementary therapy in the treatment of TBI. This note explores its mechanisms, efficacy, and future directions for Neurofeedback in TBI treatment 
Understanding Neurofeedback
Neurofeedback, also known as EEG biofeedback, is a non-invasive therapeutic intervention that teaches self-regulation of brain function by providing immediate feedback on brainwave activity. It leverages operant conditioning, where individuals learn to modify their brainwave patterns through visual or auditory cues, such as a video game responding to increased alpha waves. Brainwaves are categorized into frequency bands, each associated with specific mental states:
- Delta waves (0.5-4 Hz): Linked to deep sleep and unconsciousness.
- Theta waves (4-8 Hz): Associated with relaxation, creativity, and meditation.
- Alpha waves (8-12 Hz): Indicate a calm, focused state.
- Beta waves (12-30 Hz): Reflect active, alert states.
- Gamma waves (above 30 Hz): Involved in high-level cognitive processing.
This process, practiced for over six decades, aims to address symptoms by enhancing brain plasticity and self-regulation, as noted in guidelines from the International Society for Neurofeedback and Research (What is Neurofeedback?).
Understanding Traumatic Brain Injury
TBI is defined as damage to the brain caused by an external force, such as a blow or jolt to the head, leading to a range of symptoms from mild (e.g., headaches, dizziness) to severe (e.g., prolonged unconsciousness, coma). The National Institute of Neurological Disorders and Stroke outlines that TBI can result in primary injuries from mechanical forces and secondary injuries from subsequent biochemical processes, affecting neurons, axons, and blood vessels (Traumatic Brain Injury (TBI)). Common symptoms include memory loss, difficulty concentrating, mood swings, and sleep disturbances, significantly impacting quality of life.
Research indicates TBI alters brainwave patterns, with studies showing increased slow wave activity (delta, theta) and decreased fast wave activity (beta, gamma), as seen in a 2023 article from Horizon TBI & Brain Center, noting disrupted patterns affecting cognitive processes (The effects of brainwave activity with a TBI). These changes can persist, contributing to chronic symptoms.
Mechanisms of Neurofeedback for TBI
Neurofeedback for TBI begins with an EEG assessment to map brainwave abnormalities, such as excessive theta waves indicating slowed activity or reduced beta waves linked to attention deficits. The therapy then employs customized protocols to target these dysregulations, aiming to normalize brain function. The process involves:
- Initial Assessment: Using EEG to identify specific frequency band imbalances, often guided by quantitative EEG (qEEG) for precision, as discussed in a 2003 analysis by Collura and Ayers (Quantitative electroencephalographic (qEEG) normative databases).
- Training Sessions: Patients undergo 20-40 sessions, typically 30-60 minutes each, where they receive real-time feedback. For instance, if targeting increased alpha waves for relaxation, a pleasant sound or visual effect rewards the desired activity, reinforcing self-regulation, as described in a 2024 Britannica article (Neurofeedback).
- Learning and Adaptation: Through operant conditioning, the brain learns to maintain these patterns, leveraging neuroplasticity to create new neural pathways, potentially reducing symptoms like memory issues and emotional instability.
Specific protocols include:
- Alpha-Theta Training: Increases alpha for relaxation and decreases theta to improve attention, often used for anxiety and cognitive deficits.
- SMR (Sensorimotor Rhythm) Training: Enhances beta activity in the sensorimotor cortex, aiding motor control and reducing impulsivity.
- qEEG-Guided Neurofeedback: Tailors interventions based on individual brain maps, addressing localized abnormalities.
This approach aligns with findings that TBI disrupts oscillatory rhythms, with low-frequency stimulation improving cognitive outcomes, as noted in a 2016 Frontiers article (Making Waves in the Brain).
Research and Evidence
The evidence for Neurofeedback in TBI is promising but emerging, with several studies reporting positive outcomes. A 2014 review in the Journal of Neurotrauma found Neurofeedback improved attention, memory, and mood, though it highlighted the need for more rigorous studies due to methodological limitations (Schoenfeld & Pothmann, 2014). A 2016 pilot study in the Journal of Head Trauma Rehabilitation showed cognitive and emotional benefits in veterans, with reduced depression and anxiety scores (Nelson et al., 2016). A 2009 case study demonstrated a patient with mild TBI improved verbal and visual memory after 20 sessions, suggesting efficacy for cognitive functions (Singh et al., 2009).
However, challenges include small sample sizes, lack of placebo-controlled trials, and variability in protocols, as noted in a 2013 PubMed review, calling for double-blind studies to determine its role (Hammond, 2013). Despite these, a 2023 meta-analysis on related conditions like PTSD suggests Neurofeedback’s potential, indicating broader applicability (Askovic et al., 2023).
Case Studies and Real-World Impact https://healingthehero.org/testimonials/
Real-world examples provide insight into Neurofeedback’s practical benefits. A 35-year-old male with moderate TBI from a motorcycle accident, reporting concentration and memory issues, underwent 30 sessions targeting alpha and beta waves, noting significant focus and recall improvements, as per a case study from the Center for NeuroPotential (Neurofeedback Case Studies). Another case involved a 42-year-old female with severe TBI from a car accident, experiencing chronic pain and depression; after sessions reducing theta activity, she reported reduced pain and better mood, highlighting emotional regulation potential.
These anecdotes, while not scientific evidence, align with clinical observations from the Drake Institute, which has used Neurofeedback for 40 years, reporting long-term symptom relief without drugs (Neurofeedback For Traumatic Brain Injuries).
Now let me share my TBI story. TBI has been an ongoing issue in my life, my first TBI was at 6 years old riding a bike with no helmet. We did that back in the day circa 1976 when my dad was a Navy recruiter in Michigan. Just a few years fast forward and I started playing football in the third grade, Little League was a blast, literally. Then middle school football and then High School football. I haven’t even gotten to the Army yet. Wrestling in High School brought numerous slams where stars could be seen. in 1993 I had a head on collision in a car crash, 1995 a rear end collision, my rear end of my Mustang. Now let’s discuss Deployments, one in 2006-2007 (15 Months) this Iraq deployment had my bell get rung a few times from bast injuries. One at the end of my deployment was a 122mm artillery round detonating atop of a HESCOE barrier maybe 15 feet from me, one more foot into our Patrol Base Millet and I would’t be hear to share this story. Let’s fast forward to Afghanistan in 2012 (12 months) 3 TBIs in close proximity, an air burst 82mm recoilless rifle or RPG unknown which knocked me, my platoon sergeant and another squad leader to the ground, this was March 2011. Not long after this in June 2011 a 250 pound Stryker hatch dropped onto my skull with no helmet, that stung. Then in July 2011 I stepped on a Pressure Plate while on a dismounted patrol leading four Americans, four Afghans and one interpreter across the Tarnac River in Zabul Province of Afghanistan. I stepped on a pressure plate and detonated an Improvised Explosive Device (IED) that was only 10 feet away. This one caused me to get a Purple Heart as I had no say in the matter. The deployments ended as did the career by September 11, 2014 and wouldn’t you know it back in Florida two weeks later a vehicle rollover. We tumbled 3 times and landed upright in a beautiful 2006 Ford F350 Diesel Truck. I loved that truck, but the cage saved me for sure. Now you know why I wanted to throat punch the VA Doctor.
Evoke NeuroScience and Dr. David Hagedorn
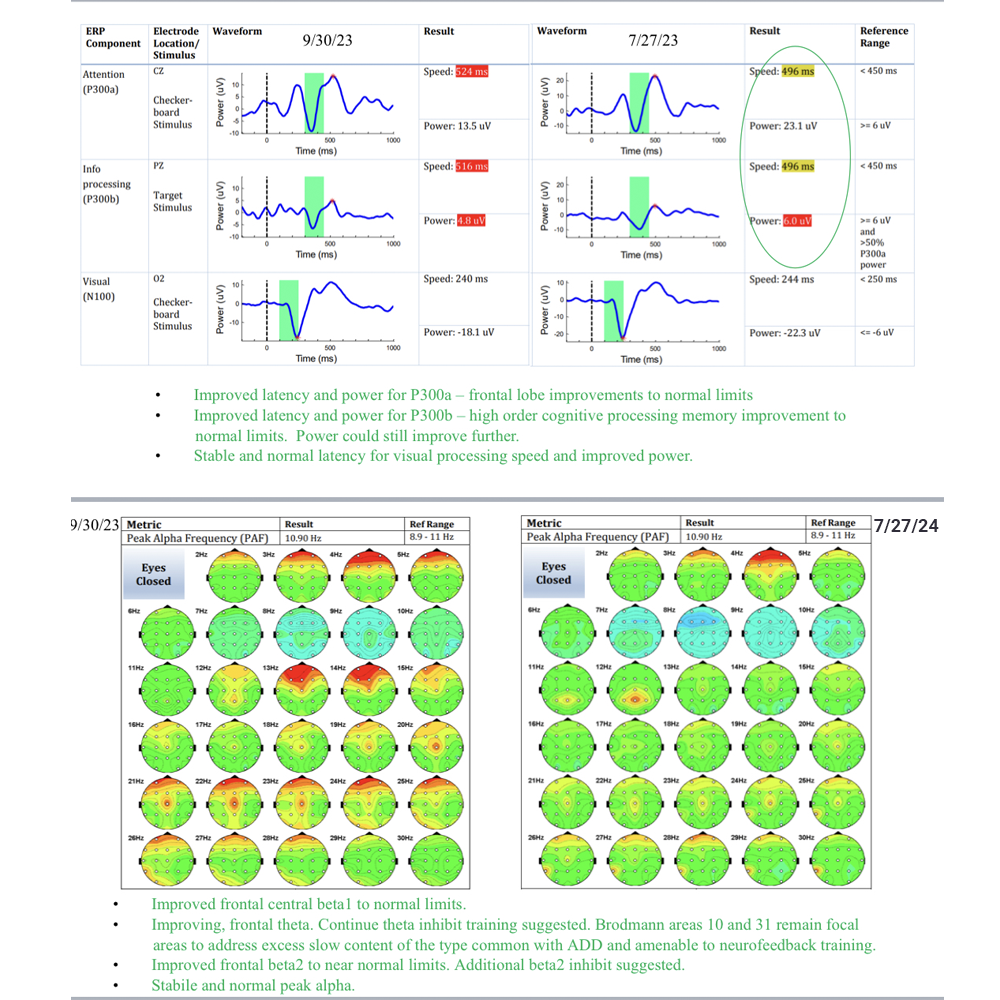
Dr. Hagedorn met with me and did my first brain scan and it answered a lot of questions. To the point I stopped and looked at Dr. hagedorn when he told me what my symptoms more than likely were based on what he saw on the qEEG. “Did you have a camera in my house for the past decade?” I asked. Finally someone willing to listen and help. He said there is a fair amount of TBI damage related to frontal lobe and top brain. Emotional Dysregulation, Decision making problems (logic) and impulse control. I wondered why I kept buy high dollar rifles like a Tavor 7 with an Acog, coming in at $3500, and a Kris Vector with a Suppressor and SBR, Eotech scope registering in at another $3500, like I needed them. They were cool but just adding to a collection i can’t take with me when this world ends for me. Very impulsive behavior. Fast forward 7 months of NeuroFeedback, sleep has restored, emotions have regulated and the impulse control has resolved. The qEEG scan post NeuroFeedback shows a remarkable improvement with the brain.
Potential Risks and Considerations
Neurofeedback is generally safe, with minimal side effects like temporary headaches, dizziness, or fatigue, as noted in a 2021 New York Times article (What to Know About Neurofeedback Therapy). However, ensuring sessions are conducted by trained professionals is crucial, given the complexity of TBI. It should complement, not replace, conventional treatments like physical therapy or medication, as emphasized in a 2023 Verywell Mind article (What to Know About Neurofeedback Therapy).
Patients with severe TBI or comorbidities like active psychosis may require additional evaluation, as per exclusion criteria in some studies, ensuring safety and efficacy.
Implementation Strategies
Implementing Neurofeedback for TBI involves:
| Strategy | Description |
| Initial Assessment | Conduct EEG and qEEG to map brainwave patterns, identifying targets for training. |
| Customized Protocol Design | Develop specific protocols based on assessment, such as alpha-theta or SMR training. |
| Session Scheduling | Plan 20-40 sessions, 30-60 minutes each, with regular progress evaluations. |
| Integration with Care | Ensure Neurofeedback complements existing treatments, coordinating with healthcare providers. |
| Monitoring and Adjustment | Regularly assess outcomes, adjusting protocols as needed based on patient response. |
Costs vary, with sessions ranging from $100-$300 each, depending on location and provider, as per a 2024 EEG Info guide (What is Neurofeedback?). Veterans with Combat Related TBI or PTSD with a service rating 70 percent or higher can get assistance from The Semper Fi & Americas Fund and their NeuroFit program. Click here to learn more. https:/thefund.org/our-programs/integrative-wellness-program/neurofitness/
Conclusion
Neurofeedback offers a promising, non-invasive approach to manage TBI symptoms, leveraging brain plasticity to improve cognitive and emotional outcomes. While current evidence is encouraging, further large-scale, randomized controlled trials are needed to refine protocols and confirm efficacy. As research advances, it may become a standard complementary therapy, enhancing quality of life for TBI patients.
Overview of Blast-Related TBI in Combat Veterans
Since September 11, 2001, combat operations in Iraq and Afghanistan have led to a significant number of blast-related TBIs among US military personnel. Research suggests that approximately 168,600 veterans have experienced blast-related TBI, calculated from 33.1% of the 509,477 total TBIs reported by the Department of Defense from 2000 to the second quarter of 2024, adjusted for the post-9/11 period.
VA’s Efforts to Address Blast-Related TBI
The Department of Veterans Affairs (VA) is actively working to support veterans with blast-related TBIs through various programs. These include the Translational Research Center for TBI and Stress Disorders (TRACTS), which studies long-term effects and develops new treatments, and the Chronic Effects of Neurotrauma Consortium (CENC), a joint initiative with the Department of Defense. Additionally, the Long-Term Impact of Military-Relevant Brain Injury Consortium (LIMBIC-CENC) focuses on the chronic effects of mild TBI, with many participants having blast-related injuries. The VA has also introduced a new ICD-10 code for primary blast injury to improve tracking and care. Yet they do not offer NeuroFeedback as of yet. Take it from me, when I initially reported to the VA in 2014 upon my retirement from the U.S. Army, a young Doctor looked at me and smirked and then said something that shocked me, “What’s the big deal it’s just a concussion.” I wanted to throat punch him, and I just had to walk out.
Problems Arising from TBI in Veterans
TBI can lead to a range of issues, especially for veterans. Common problems include memory loss, difficulty concentrating, headaches, and mood swings, which can significantly impact daily life. Veterans may also face increased risks of depression, anxiety, and post-traumatic stress disorder (PTSD), compounded by their combat experiences. These challenges can affect relationships, employment, and overall well-being, making effective treatment crucial.
Unexpected Detail: High Incidence in Modern Warfare
An interesting aspect is that blast injuries, often from improvised explosive devices (IEDs), have become a signature injury of modern warfare, with up to 80% of TBIs in Iraq and Afghanistan linked to blasts, highlighting the unique challenges faced by post-9/11 veterans compared to earlier conflicts.
Article by: Dan Jarvis | Founder of TRUSA, 22ZERO and Healing the Hero.