
Table of Contents
Abstract
This case study examines psychological, cognitive, and neurophysiological outcomes in a 28-year-old male following Trauma Resiliency Protocol–Peer Rescue (TRP-PR). Baseline measures indicated moderate trauma burden (Posttraumatic Stress Disorder Checklist for DSM-5 [PCL-5] = 46), mild depressive symptoms (Patient Health Questionnaire-9 [PHQ-9] = 9), and mild anxiety (Generalized Anxiety Disorder-7 [GAD-7] = 6). Neurophysiological assessment using the Evoke Neuroscience system revealed a global neurocognitive score of 83%, affect dysregulation, slightly slowed processing speed, and an elevated theta: beta ratio. Following intervention, psychometric scores decreased to zero across all measures (PCL-5, PHQ-9, GAD-7), and global neurocognitive performance improved to 100%. Findings demonstrate rapid symptom resolution accompanied by measurable cognitive and electrophysiological changes.
Introduction to Emotional Recovery
Law enforcement professionals operate in occupational environments defined by repeated exposure to violence, human suffering, threat, uncertainty, and cumulative operational stress. These exposures are not episodic anomalies in policing; they are embedded features of the profession. As a result, police officers are at increased risk for trauma-related symptoms, depression, sleep disruption, irritability, emotional numbing, and impaired recovery when compared with the general population (Violanti et al., 2017).
The literature suggests that trauma-related symptom burden in law enforcement is substantial, though prevalence estimates vary depending on methodology, population, and threshold definitions. In a systematic review of police officers exposed to routine work-related critical incidents, Wagner et al. (2020) concluded that posttraumatic stress disorder (PTSD) prevalence in police populations is elevated and highly associated with occupational exposure. Nationally, the operational risk burden remains high. According to the Federal Bureau of Investigation (2024), 79,091 officers were assaulted in the line of duty in 2023, the highest officer assault rate reported in the past 10 years. These figures reinforce that repeated exposure to danger and violence remains a defining aspect of law enforcement service.
The psychological burden appears to extend beyond diagnosable PTSD alone. In a survey study of 434 officers from a large urban police department, Jetelina et al. (2020) found that 26% screened positive for current mental illness symptoms, including depression, anxiety, PTSD, or suicidal ideation/self-harm symptoms, while only a minority had sought mental health services. This gap between symptom burden and treatment engagement has major implications for early intervention and operational readiness.
For early-career officers, the impact of a severe line-of-duty assault may be particularly destabilizing. Such incidents may create both acute trauma responses and cumulative changes in hypervigilance, sleep, anger regulation, and physiological stress activation. In cases where the officer remains outwardly functional, clinically meaningful trauma burden may still persist internally, affecting emotional regulation, decision efficiency, and long-term wellness.
Trauma Resiliency Protocol–Peer Rescue (TRP-PR) is intended to address unresolved emotional injury through a brief, structured intervention that does not depend on prolonged verbal reliving of the traumatic event. The present de-identified case study evaluates psychological, neurocognitive, and neurophysiological outcomes in a law enforcement officer with three years of service who survived a near-death line-of-duty beating. Neurophysiological assessment was conducted using the Evoke Neuroscience system, which integrates quantitative electroencephalography (qEEG), event-related potentials (ERPs), electrocardiography (ECG)-derived heart rate variability (HRV), and a computerized neurocognitive screener. TRUSA IP Owners of TRP-PR
Method
Participant
- Age: 27 years (pre-intervention), 28 years (post-intervention)
- Sex: Male
- Occupation: Law enforcement officer with three years of service
- Index trauma: near-death line-of-duty assault involving a severe physical beating
- Presenting symptoms: sleep disruption, increased anger reactivity, fear responses when reminded of the event, and depressive symptoms
- Active Duty Naval Special Warfare Operator Case Study
Measures
- Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5)
- Patient Health Questionnaire-9 (PHQ-9)
- Generalized Anxiety Disorder-7 (GAD-7)
- Evoke Neuroscience platform (EEG, ERP, HRV, neurocognitive screener)
Procedure
The participant completed baseline psychometric and Evoke Neuroscience assessments prior to intervention. He then completed three sessions of Trauma Resiliency Protocol–Peer Rescue (TRP-PR), a structured trauma-processing intervention designed to reduce the emotional intensity associated with unresolved traumatic experiences without requiring prolonged narrative exposure. Following completion of the three-session intervention, the participant underwent post-intervention reassessment using the same psychometric and neurophysiological measures.
Results
Psychometric Outcomes
| Measure | Pre | Post | Change |
| PCL-5 | 46 | 0 | -46 |
| PHQ-9 | 9 | 0 | -9 |
| GAD-7 | 6 | 0 | -6 |
Neurocognitive Performance
- Global Score improved from 83% to 100%
Domain-Level Changes
- Affect: 42% → 100%
- Executive Function & Attention: 58% → 100%
- Memory: maintained at 100%
- Sensory and Motor domains: improved to 100%
These changes reflect a transition from partial emotional and executive inefficiency to fully optimized performance across all measured domains.
Response Metrics
| Metric | Pre | Post | Interpretation |
| Reaction Time | 530ms | 721ms | Slower post-intervention |
| Response Consistency | 5ms | 5ms | Stable and optimal |
| Omission Errors | 0% | 0% | No attentional lapses |
| Commission Errors | 0.41% | 0% | Slight improvement |
The increase in reaction time may reflect more deliberate processing rather than impairment, particularly given the absence of errors and perfect cognitive domain scores post-intervention.
ERP Findings
| ERP Component | Pre | Post | Interpretation |
| P300a (Attention) | 484ms | 460ms | Improved processing speed |
| P300b (Information Processing) | 520ms | 500ms | Improved efficiency |
| N100 (Sensory Processing) | Measurable | Indiscernible | Reduced signal clarity post-test |
Overall, ERP data suggest improved higher-order processing speed (P300), with mixed findings in early sensory processing (N100).
HRV Findings
| Metric | Pre | Post | Interpretation |
| SDNN | 56ms | 49ms | Slight decrease |
| Total Power | 1319 ms² | 1146 ms² | Slight decrease |
| Heart Rate | 76 bpm | 80 bpm | Within range |
Although HRV metrics declined slightly, they remained within a functional range. These changes may reflect scan conditions, recent activity, or transient physiological factors rather than reduced recovery.
qEEG Findings
Baseline analysis showed an elevated theta: beta ratio (2.349), exceeding the reference threshold and suggesting increased cognitive or emotional load. Posterior regions demonstrated excess activity patterns consistent with heightened internal processing.
Post-intervention analysis showed a slight reduction in theta: beta ratio (2.317) and a more stable cortical distribution. While still slightly elevated, the overall pattern suggests improved neural efficiency and reduced dysregulation.
Intervention Overview
TRP-PR was delivered across three sessions. Core intervention components included:
- guided dissociation from distressing sensory imagery,
- reduction of trauma-linked emotional intensity,
- memory reconsolidation strategies,
- emotional reframing, and
- future-oriented state stabilization.
The protocol was designed to reduce emotional interference while preserving cognitive integrity and promoting adaptive emotional processing.
Discussion
Key Findings
This case demonstrated:
- Complete resolution of trauma, depression, and anxiety symptoms
- Full optimization of neurocognitive performance (83% to 100%)
- Significant improvement in affect regulation and executive function
Interpretation
Unlike severe trauma cases, this participant presented with relatively intact baseline cognition but clear emotional dysregulation. TRP-PR appears to have reduced emotional interference, allowing existing cognitive capacity to function at its full potential.
Processing Speed Consideration
The increase in reaction time, despite improved outcomes in all other domains, suggests a shift toward more controlled and deliberate processing rather than impulsive responding. This may represent improved cognitive regulation rather than decline.
Autonomic Considerations
HRV findings did not mirror subjective and cognitive improvements. This reinforces the concept that emotional and cognitive recovery can precede full autonomic regulation. External variables such as sleep, hydration, stress exposure, and testing conditions may influence HRV independently of treatment outcomes.
Conclusion
This case supports TRP-PR as an effective brief intervention for moderate trauma presentations. Following three TRP-PR sessions, the participant demonstrated rapid elimination of psychological symptoms, full cognitive optimization, and measurable neurophysiological shifts. The participant demonstrated rapid elimination of psychological symptoms, full cognitive optimization, and measurable neurophysiological shifts following intervention.
The findings suggest that TRP-PR may be particularly effective in cases where emotional dysregulation, rather than cognitive impairment, is the primary limiting factor.
Appendix A
Figure A1. Pre-Intervention Evoke Eyes-Closed qEEG Brain Map
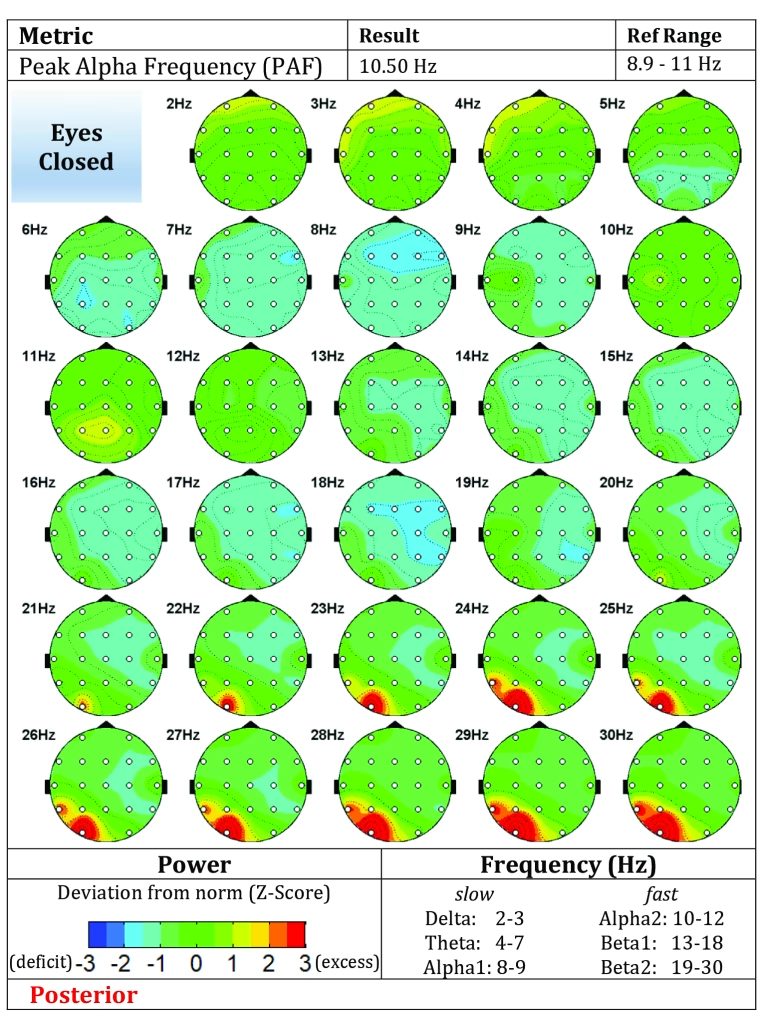
caption: Baseline Evoke Neuroscience qEEG demonstrating elevated posterior excess activity and increased theta: beta ratio consistent with elevated cognitive-emotional load.
Figure A2. Post-Intervention Evoke Eyes-Closed qEEG Brain Map
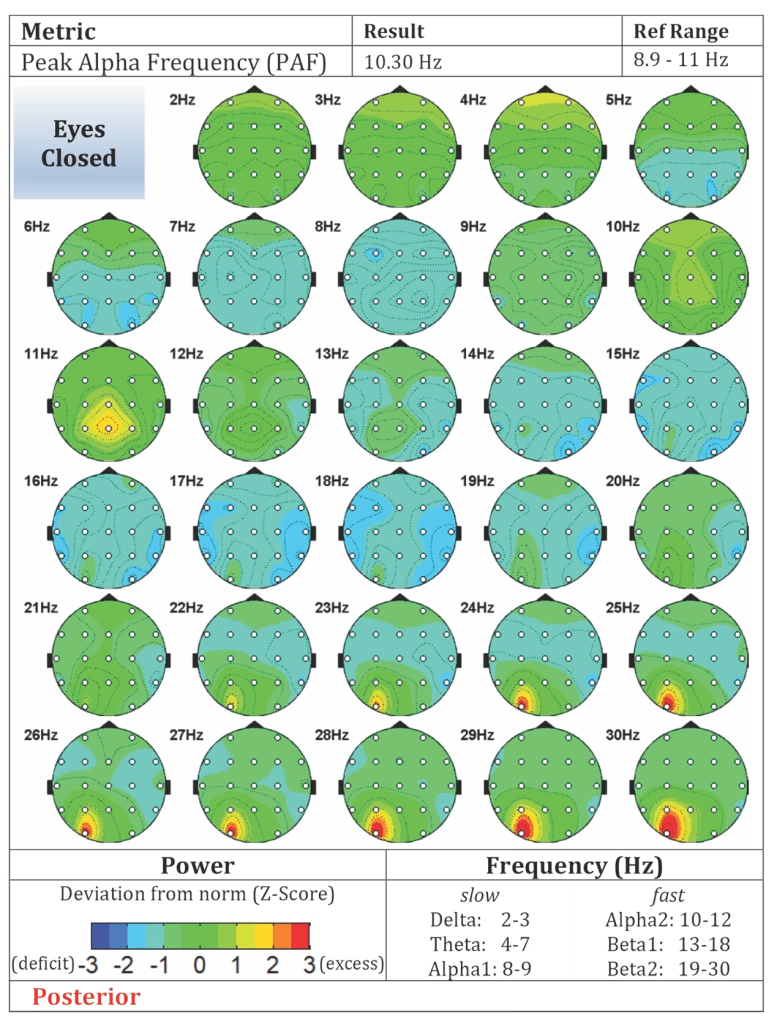
caption: Post-treatment Evoke Neuroscience qEEG demonstrating improved cortical organization and reduced excess activity following three TRP-PR sessions.
Figure A3. Pre/Post Outcome Summary Table – side-by-side summary:
- PCL-5: 46 → 0
- PHQ-9: 9 → 0
- GAD-7: 6 → 0
- Global Cognitive Score: 83% → 100%
- Affect: 42% → 100%
- Executive Function: 58% → 100%
Appendix Note. Appendix materials are intended to provide visual support for the psychometric, neurocognitive, and neurophysiological findings presented in the main manuscript.
References
Dawson, J. (2019, April 8). Fighting stress in the law enforcement community. National Institute of Justice. https://nij.ojp.gov/topics/articles/fighting-stress-law-enforcement-community
Evoke Neuroscience. (n.d.). Evoke EEG system documentation.
Federal Bureau of Investigation. (2024, May 14). FBI releases officers killed and assaulted in the line of duty, 2023 special report and law enforcement employee counts. https://www.fbi.gov/news/press-releases/fbi-releases-officers-killed-and-assaulted-in-the-line-of-duty-2023-special-report-and-law-enforcement-employee-counts
Jetelina, K. K., Molsberry, R. J., Gonzalez, J. R., Beauchamp, A. M., & Hall, T. (2020). Prevalence of mental illness and mental health care use among police officers. JAMA Network Open, 3(10), e2019658. https://doi.org/10.1001/jamanetworkopen.2020.19658
Violanti, J. M., Charles, L. E., McCanlies, E., Hartley, T. A., Baughman, P., Andrew, M. E., Fekedulegn, D., Ma, C. C., Mnatsakanova, A., & Burchfiel, C. M. (2017). Police stressors and health: A state-of-the-art review. Policing: An International Journal, 40(4), 642–656. https://doi.org/10.1108/PIJPSM-06-2016-0097
Wagner, S. L., White, N., Fyfe, T., Matthews, L. R., Randall, C., Regehr, C., White, M., Alden, L. E., Buys, N., Carey, M. G., Corneil, W., Fraess-Phillips, A., Krutop, E., & Fleischmann, M. H. (2020). Systematic review of posttraumatic stress disorder in police officers following routine work-related critical incident exposure. American Journal of Industrial Medicine, 63(7), 600–615. https://doi.org/10.1002/ajim.23120
Article by: Dan Jarvis | Founder of TRUSA, 22ZERO and Healing the Hero.